
.png)
COPD - "Starts silently-catch it before it catches you"
- Bharat Chukka
- Aug 31, 2025
- 4 min read


COPD CAN BE COMPLEX!!
CATCH IT EARLY, CONTROL IT BETTER AND BREATHE EASY .
WHAT IS COPD?
COPD is a Chronic Obstructive Pulmonary Disease which progresses over years. It includes CHRONIC BRONCHITIS and EMPHYSEMA or BOTH.
WHAT IS THE BURDEN OF COPD?
COPD is now one of the TOP three causes of death worldwide.
About three million people die every year. In India alone half a million die due to COPD every year. About 55 to 60 million people in India live with COPD.
WHAT CAUSES COPD?
95% of COPD cases are smoking related, typically occuring in persons of > 35 years of age with history of 10 to 20 pack years of cigarette smoking. Other types of tobacco like pipe, beedi, cigar, water pipe, marijuana are also risk factors for COPD. Other risk factors are biomass fuel like coal , animal dung cakes, dry grass ,dusts,pollutants, fumes and chemicals. Frequent childhood respiratory infections, poorly controlled asthma in childhood may cause developement of COPD in adulthood. Rarely genetic disorders like alpha 1 antitrypsin deficiency can also cause COPD in young age..
HOW TOXIC IS TOBACCO SMOKE?

Cigarrete smoke is a mixture of over 4000 chemical compounds which include 70 known carcinogens. Though nicotine is resposible for cigarrete addiction ,the more harmful substances toxic to lung are Tar, Carbonmonoxide, Hydrogen cyanide, Benzene, Formaldehyde, and Radio active elements like Polonium-210.
HOW DOES THE SMOKE DAMAGE THE LUNG ?
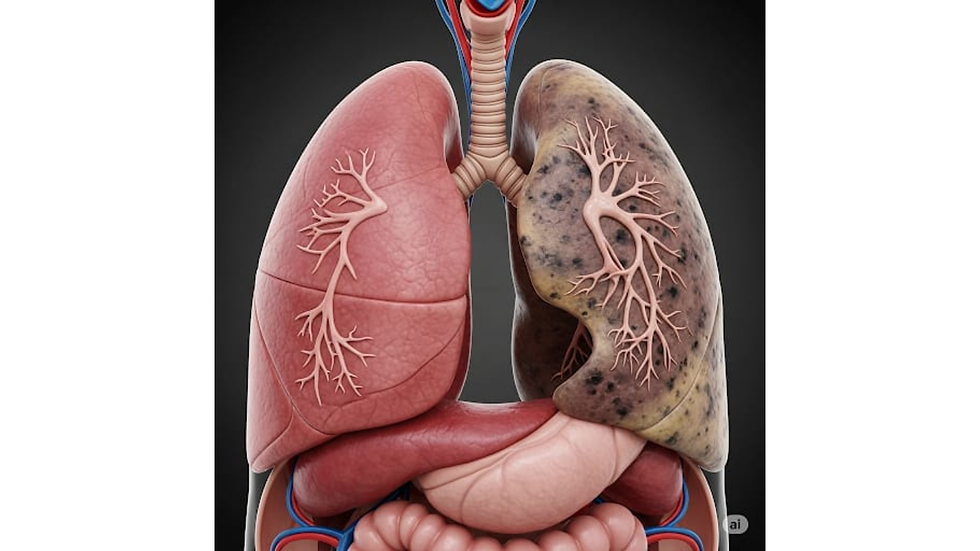
The toxic chemicals in smoke cause damage to lung tissue leading to air flow obstruction, making breathing difficult. In CHRONIC BRONCHITIS, there is enlargrment of mucus glands with mucus hypersecretion, destruction of airway cartilage, loss of function in mucosal cilia resulting in narrowing of small air ways .In EMPHYSEMA there is destruction of air sacs ,causing permant dialatation of airspaces and loss of natural elastic recoil. Generally both features are present in COPD. Altogether there is resistance to airflow in airways, resulting in difficulty in expelling air out.
THERE IS NO "SAFE LEVEL" OF SMOKING.
STOPPING COMPLETELY IS THE BEST THING ONE CAN DO TO IMPROVE LUNG HEALTH.
WHY IS COPD CALLED "A DISEASE OF ACCLERATED AGEING" ?

Normally as the age increases (in non smokers), there is gradual decline in lung function. The FEV1 ( forced expiratory volume in one second, an important lung function) in elderly non smokers, falls at a velocity of 30 ml / year, due to changes with ageing. Where as, in a COPD patient,the same FEV1 falls at a velocity of about 66.3 ml/ year ( double volume). The changes of loss of elastic recoil of lung, airwall thickening and reduced repair capacity, all begining at an early age in a smoker. This makes a COPD patient 'BIOLOGICALLY OLDER ' than his CHRONOLOGOCAL AGE . Therfore COPD can be called as a disease of ACCELERATED AGEING.
WHAT ARE THE GENERAL COMPLAINTS OF A COPD PATIENT WHEN HE VISITS A PULMONOLOGIST/ CHEST SPECIALIST?

BREATHLESSNESS, which progresses over time ,gets worse with exercise , and becomes persistent in later years.
CHRONIC COUGH, productive or non productive,
WHEEZE ( musical sounds from lungs)
RECURRENT RESPIRATORY INFECTIONS with exaggerated symptoms
IF UNTREATED, the disease will progress to right heart failure, manifesting as ankle edema,puffy eyelids and conjunctival suffusion.
HOW DOES A PULMONOLOGIST DIAGNOSE COPD?
SPIROMETRY is the key diagnostic test for COPD.
A POST BRONCHODIALATOR FEV1/FVC (Forced Expiratory Volume in 1 sec / Forced Vital Capacity) < .7
Increased lung volumes like FRC,RV,TLC and decreased DLCO support the diagnosis.
CHEST XRAY: May reveal hyperinflated (increased volume) lungs, flat diaphragm, horizontal ribs and Bullae (huge air containing spaces in lung paranchym)
Checking Alpha1 Antitrypsin levels in young adults presenting with COPD.
HOW IS COPD MANAGED?
All smokers should be strongly encouraged to QUIT SMOKING by councelling.
NICOTINE REPLACEMENT THERAPY /NRT : (gum, mint,patches,lozenges) as advised by the Pulmonologist , making it simpler to quit cigarettes.
PHARMACOLOGICAL MANAGEMENT.

KEY COPD MEDICATIONS ARE THROUGH INHALATION THERAPY:
INHALED BRONCHODIALATORS ARE:
Short Acting Beta2Agonists( SABA) or Short Acting Muscarinic Antagonists (SAMA)
for quick relief ( RESCUE INHALERS)
eg. Salbutamol, Terbutaline,Ipratropium
Long Acting Beta2 Agonists (LABA) and Long Acting Muscarinic Antagonists(LAMA) for prolonged relief.
eg. Salmeterol, Formoterol,Vlanterol,Indacaterol,Olodaterol(LABA)
AND
Tiotropum , Glycopyrronium,Umeclidinium,Aclidinium,Revefenacin.(LAMA)
INHALED ANTI INFLAMMATORY MEDICINES ARE :
INHALED CORTICOSTEROIDS( ICS) :
Budesonide,Beclomethasone,Fluticasone etc.
INHALER DEVICES: vary from Metered Dose Inhaler(MDI), Dry Powder Inhaler(DPI),
Soft Mist Inhaler(SMI) to Nebuliser.
The choice of INHALED BRONCHODILATOR AND INHALED ANTI INFLAMMATORY THERAPY ( LABA/LAMA/ICS or the combinations- TRIPLE THERAPY with LABA+LAMA+ICS ) and the Inhaler device will be decided by the Consultant Pulmonologist/Chest Specialist, according to the severety of COPD and comfort of the patient.
OTHER MEDICATIONS FOR COPD INCLUDE:
Oral methylxanthines (theophyllin), Phosphodiesterase 3 & 4 inhibitors like Roflumilast,Ensifentrine , Biologic drug like Dupilumab and Mucolytics and Anti oxidants like Carbocysteine,Erdosteine, N-Acetylcysteine.
In advanced COPD cases, Home oxygen therapy for hypoxemic patients, NIV support in acute or chronic respiratory failure..
NONPHARMACOLOGICAL MANAGEMENT :
Pulmonary Rehabilitation, Exercise training, Nutritional support.
VACCINATIONS:
Influenza vaccine annually and Pneumococcal vaccination ,RSV vaccinations
Others are Covid19 vaccination,Shingles and Pertussis vaccinations.
IS THERE ANY ROLE FOR SURGERY IN SEVERE COPD?
BULLECTOMY :
Large bullae with trapped air can be excised by surgery.
LVRS: LUNG VOLUME REDUCTION SURGERY:
In this, small amount of damaged lung tissue is removed so that healthy lung can expand and oxygenation is better.
LUNG TRANSPLANTATION:
In advanced COPD patients, one or both of the lungs are replaced with a Donor's lungs. It improves quality of life but may not have significant increase in survival.
WHAT ARE THE LATEST TREATMENTS AVAILABLE IN COPD?

Thanks to medical advances, there are new options to help people with severe COPD.
They are:
BTVA (Bronchoscopic Thermal Vapor Ablation):
Throgh bronchoscope, a special device is used to deliver heated water vapor or steam into damaged areas of lung. The steam causes diseased parts to shrink, making more room for healthier lung to function better.
TLD (Targeted Lung Denervation):
In this, Pulmonologist uses bronchoscope and special radiofrequency energy to disrupt the nerves in the airways which are responsible for airway narrowing. It helps to reduce symptoms like constant coughing.
ELVR (ENDOSCOPIC LUNG VOLUME REDUCTION) OR BLVR :
The bronchoscopist places tiny one way valve in the airways. It allows trapped air to be absorbed making it easier for rest of the lung to function better.
Others are coil placement,bypass stents and sealants.
These procedures donot involve major surgery and show promising results.
COPD REMAINS INCURABLE .
BUT IS INCREASINGLY MANAGEABLE .
WITH ADVANCES IN PHARMACOLOGIC AND SUPPORTIVE CARE ;
HOPEFULLY IMPOOVING QUALITY OF LIFE AND
REDUCING FREQUENCY OF EXACERBATIONS.



Comments